All published articles of this journal are available on ScienceDirect.

Systematic Review and Meta-Analysis of the Effects of Aged Garlic Extract on Cardiovascular Diseases
Authors Info & Affiliations
Abstract
Introduction
Cardiovascular Diseases (CVDs) continue to be the leading cause of death globally, which highlights the need to evaluate nutraceuticals like Aged Garlic Extract (AGE) for risk factor management. This systematic review and meta-analysis compiles the data on how AGE affects blood pressure, lipid profiles, inflammation, and glycaemic control in adults at risk for CVD.
Methods
PRISMA guidelines were followed when searching databases (PubMed, Cochrane CENTRAL, Google Scholar) for randomized, double-blind, placebo-controlled trials from the beginning to May 2025. Research that was observational or crossover was not accepted. Standardised Mean Differences (SMDs) with 95% Confidence Intervals (CIs) were calculated using random-effects models, and the risk of bias was assessed using Cochrane tools.
Results
Systolic (-1.71 mmHg, p = 0.54) and diastolic (-0.77 mmHg, p = 0.44) blood pressure decreased non-significantly in ten trials (n = 625), with dose-dependent trends (e.g., -1.25 mmHg SBP at ≤ 1200 mg/day). Triglycerides trended lower (-22.08 mg/dL, p = 0.24), and TNF-α dropped significantly (-178.62 fg/mL, p = 0.02). Heterogeneity was low-moderate for lipids/inflammation (I2 = 0-64.65%) but high for blood pressure (I2 = 87.39%).
Discussion
AGE marginally decreases cardiovascular risk factors, particularly inflammation (TNF-α), but has variable, dose-dependent effects upon blood pressure and cholesterol. Inconsistent doses and heterogeneity of the studies prevent definitive conclusions; future studies should use a standardised protocol.
Conclusion
There are dose-dependent cardiovascular benefits to supplementation with AGE, including reductions in TNF-α and possibly blood pressure and cholesterol. Larger, standardised studies are required to optimize the dosage for high-risk populations. Registered in PROSPERO (CRD420251033175).
1. INTRODUCTION
Despite advances in prevention and treatment approaches that have aided in a gradual decline in morbidity and mortality in the past 40 years, Cardiovascular Disease (CVD) continues to be the leading cause of death in developed countries [1]. Given this considerable burden, there is growing interest in dietary and nutraceutical interventions to alleviate cardiovascular-related risk factors. Garlic, Allium sativum L., has increasingly gained recognition from global public health authorities for its cardioprotective effects in the context of hypertension, dyslipidemia, and chronic inflammation [2]. AGE, a modified garlic preparation resulting from prolonged (≥ 10 months) suspension of sliced and macerated garlic in an ethanol-water (70:30) mixed solution [3, 4], undergoes chemical transformation that appears to enhance its therapeutic efficacy. While raw garlic contains pungent and irritating compounds like allicin, AGE is richer in stabilized, bioavailable, and odorless sulfur-containing compounds such as S-allyl cysteine (SAC), S-Allyl Mercaptocysteine (SAMC), selenium, and allixin [5, 6]. These compounds exhibit antioxidant and anti-inflammatory activity, and AGE contains more than twice the total phenolic content (129 ± 1.8mg/g) of fresh garlic (56 ± 1.2 mg/g) [7]. As a result, AGE is recognized as a safer and more tolerable option to raw garlic, along with growing evidence for its benefit to reduce cardiovascular risk [8]. A recent meta-analysis has shown the benefit of AGE on blood pressure in hypertensive patients [9]. In particular, supplementation with AGE has demonstrated a statistically significant decrease in both systolic and diastolic blood pressure [9-12] and improved lipid profiles in hypercholesterolemic individuals, significantly reducing total cholesterol and Low-Density Lipoprotein Cholesterol levels (LDL-C) [2, 13] while increasing High-Density Lipoprotein levels (HDL-C) [14]. AGE has also been shown to modulate inflammatory pathways through reductions in pro-inflammatory cytokines, including C-Reactive Protein (CRP), Tumor Necrosis Factor-alpha (TNF- α), and Interleukin-6 (IL-6) [15, 16]. Emerging evidence has indicated AGE may improve glycemic control, supporting its possible role as an adjunct therapy for diabetes mellitus [17-19]. In addition, AGE supplementation has been associated with reduced arterial stiffness, a key indicator of vascular aging and cardiovascular risk [20-22]. Though these strong aspects of the literature are promising, we still have scattered evidence that studies have mostly examined in isolation from other cardiovascular risk factors. This meta analysis study is different from previous evidence, since it seeks to summarize and evaluate the overall effects of AGE supplementation on the key cardiovascular risk markers (i.e. blood pressure [systolic blood pressure, diastolic blood pressure, pulse pressure], lipid profile [LDL-C, HDL-C, triglycerides, total cholesterol], glycemic control [fasting blood glucose], and inflammatory biomarkers [TNF-α, IL-6, CRP]). The current study will also examine dose-response relationships and effects on patients who have cardiovascular disease risk, conducting stratified analyses based on dosage (< 1200 mg/day and ≥ 1200 mg/day) and a study period of 12 weeks. This meta-analysis aims to consolidate the existing evidence to fully assess AGE's therapeutic impact on cardiovascular disease prevention and management. This systematic review is registered in PROSPERO (ID: CRD420251033175).
2. METHODS
2.1. Data Source and Search Strategy
We conducted this systematic review and meta-analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17]. A comprehensive literature search was conducted across multiple databases, including PubMed, the Cochrane Central Register of Controlled Trials (CENTRAL), and Google Scholar, from their inception through May 2025. The search strategy incorporated both Medical Subject Headings (MeSH) terms and free-text keywords related to garlic preparations (s“garlic” OR “Allium sativum” OR “aged garlic extract” OR “Kyolic”) and cardiovascular outcomes (“cardiovascular disease” OR “hypertension” OR “endothelial function” OR “atherosclerosis”) and (“randomized controlled trial”). No restrictions were applied regarding publication language or date.
2.2. Inclusion and Exclusion Criteria
Eligible studies were randomized, double-blind, placebo-controlled clinical trials involving adults (> 18 years) at risk of CVD, assessing Aged Garlic Extract as the intervention. Exclusion criteria included observational or animal studies, crossover trials, studies involving healthy volunteers without CVD risk factors, studies lacking a placebo control, interventions using raw garlic or other garlic-based supplements, studies with insufficient data, and unpublished studies.
2.3. Data Source and Search Strategy
The extracted information from each eligible study included the title, first author’s name, year of publication, participant demographics (age and sex), design, intervention period, sample sizes, dosage of Aged Garlic Extract (AGE), and mean ± standard deviation (SD) values for outcome measures at baseline and post-intervention. The methodological quality and risk of bias of the included studies were evaluated using the Cochrane Risk of Bias tool [23].
2.4. Statistical Analysis
All analyses were performed using MedCalc Statistical Software (version 23.2.1; MedCalc Software Ltd). To calculate the overall effect size, the mean ± SD values for outcomes at baseline and post-intervention in both treatment and control groups were used. Statistical significance was defined as p-values < 0.05. Effect sizes were computed as SMDs with 95% confidence intervals, employing random-effects models. Heterogeneity was assessed using I2 statistics [Heterogeneity Index (I-square Statistics)] and p-value. Publication bias was evaluated through visual inspection of funnel plot symmetry. Sensitivity analysis confirmed no single trial skewed the pooled results.
3. RESULTS
3.1. Study Selection
Figure 1 outlines our systematic screening approach. Initially, we identified 1,149 records, of which 583 duplicates were eliminated. After deduplication, we screened the remaining 566 records by evaluating their titles and abstracts, excluding 531 irrelevant articles. Following this preliminary assessment, 35 full-text articles were selected for in-depth evaluation. Among these, 22 were discarded due to insufficient data, crossover study designs, or those that included other supplements. From the remaining 13 articles, we excluded 3 due to the lack of desired data, resulting in a final selection of 10 eligible studies for our analysis.
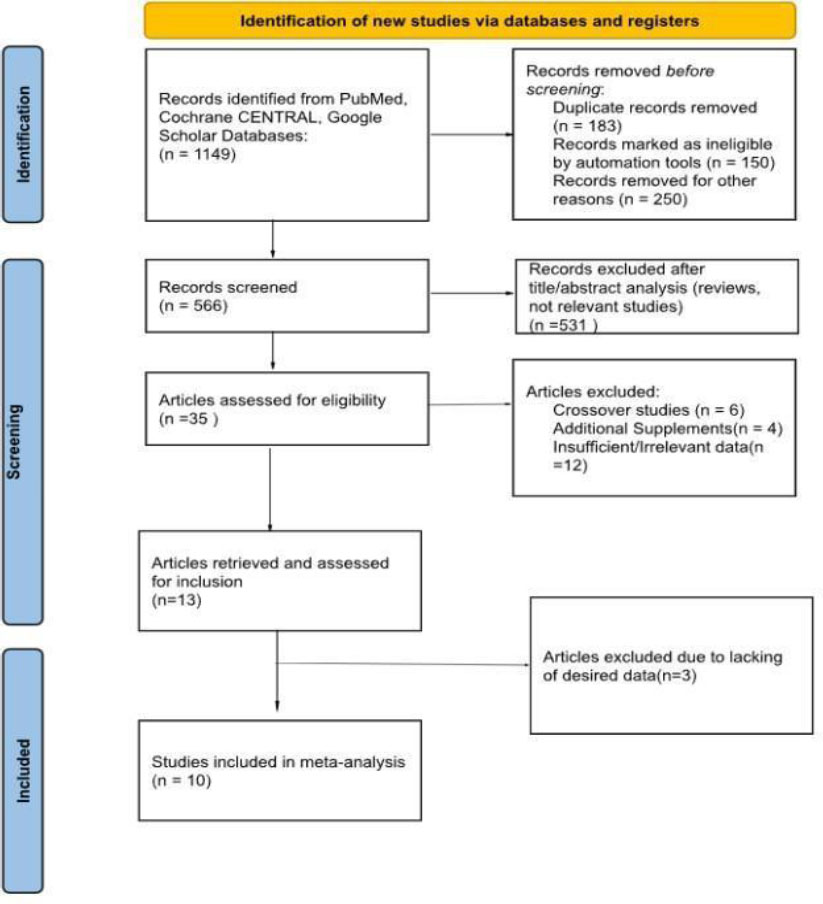
PRISMA 2020 flow diagram illustrating the study selection process for the systematic review and meta-analysis. The flowchart shows the identification, screening, eligibility assessment, and final inclusion of randomized controlled trials evaluating the effects of aged garlic extract (AGE) on cardiovascular disease-related outcomes.
3.2. Characteristics of Studies
The ten Randomized Controlled Trials (RCTs) included in this analysis, summarized in Table 1, encompassed 625 participants-316 assigned to AGE supplementation and 309 to placebo-across studies conducted from 2010 to 2024. One trial exclusively enrolled female participants. The intervention duration varied from 6 to 52 weeks, with AGE dosages ranging between 240 and 3600 mg/day. Participants had an average age of 32–82 years and a Body Mass Index (BMI) of 21–43. Based on the Cochrane risk-of-bias assessment, two studies were classified as high risk, while the rest demonstrated low risk of bias (Table 2).
| Studies/References | Year | Participants (n) | Age (years) | Gender | BMI (kg/m2) | Dose (g/day) | Duration (weeks) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | Age | Placebo | Age | M | F | M | F | Placebo | Age | Placebo | Age | ||
| Vila-Nova et al. [30] | 2024 | 10 | 9 | 47.1±6.3 | 39.5±6.8 | 6 | 4 | 6 | 3 | 33.4±5.2 | 33.7±8.06 | 1.2 | 12 |
| Ried et al. [7] | 2013 | - | - | - | - | - | - | - | - | - | - | - | - |
| Garlic 1 | - | 19 | 21 | 71.5±10.9 | 70.1±12.4 | 9 | 10 | 12 | 9 | 29.9±4.5 | 29.7±5.8 | 0.24 | 12 |
| Garlic 2 | - | 19 | 20 | 71.5±10.9 | 67.5±11.8 | 9 | 10 | 12 | 8 | 29.9±4.5 | 28.8±5.3 | 0.48 | - |
| Garlic 4 | - | 19 | 19 | 71.5±10.9 | 70.4±13.1 | 9 | 10 | 9 | 10 | 29.9±4.5 | 28.8±4.0 | 0.96 | - |
| Xu et al. [31] | 2018 | 24 | 24 | 42.4±10.7 | 45.7±12.3 | 8 | 17 | 7 | 16 | 36.3±6.0 | 36.5±6.6 | 3.6 | 6 |
| Serrano et al. [32] | 2023 | 38 | 39 | 64.1±5.9 | 63.7±5.8 | 20 | 18 | 20 | 19 | – | – | 2.25 | 12 |
| Gruenwald et al. [33] | 2019 | 29 | 26 | 57.9±10.5 | 57±7.6 | 9 | 20 | 12 | 14 | 27.69±2.03 | 28.07±2.63 | 0.06 | 12 |
| Ried et al. [34] | 2016 | 38 | 50 | 61.5±13 | 63.3±9.9 | 19 | 19 | 28 | 22 | 28.3±4.9 | 27.3±4.9 | 1.2 | 12 |
| Ried et al. [35] | 2010 | 25 | 25 | 66±9 | 66±9 | 17 | 8 | 17 | 8 | 29.1±4.7 | 31±5.8 | 0.96 | 52 |
| Wlosinska et al. [36] | 2020 | 47 | 46 | 64±6 | 63±6 | 31 | 16 | 30 | 16 | 30±4.6 | 27.6±3.7 | 2.4 | 52 |
| Ried et al. [37] | 2018 | 26 | 23 | 61.9±11.8 | 62.8±9.3 | 12 | 14 | 10 | 13 | 29.7±6.2 | 28.6±7.7 | 1.2 | 12 |
| Wlosinska et al. [38] | 2021 | 15 | 14 | 62.8±4.9 | 62.6±5.2 | 0 | 15 | 0 | 14 | 27.8±5.1 | 28.3±5 | 2.4 | 52 |
| Studies/References | Allocation Concealment | Random Sequence Generation | Blinding (Participants and Personnel) | Blinding (Outcome Assessment) | Incomplete Outcome Data | Selective Reporting | Other Bias | Overall Quality |
|---|---|---|---|---|---|---|---|---|
| Vila-Nova et al. (2024) [30] | U | L | L | U | H | L | H | Low |
| Ried et al. (2013) [7] | L | L | L | U | L | L | L | High |
| Xu et al. (2018) [31] | L | L | L | U | L | L | U | High |
| Serrano et al. (2023) [32] | L | L | L | L | L | L | L | High |
| Gruenwald et al. (2019) [33] | U | U | L | U | L | L | L | High |
| Ried et al. (2016) [34] | L | L | L | U | L | L | L | Low |
| Ried et al. (2010) [35] | L | L | L | U | L | L | L | High |
| Wlosinska et al. (2020) [36] | L | L | L | L | L | L | U | High |
| Ried et al. (2018) [37] | L | L | L | U | L | L | L | High |
| Wlosinska et al. (2021) [38] | L | L | L | L | L | L | L | High |
Note: H = High Risk of Bias, U = Unclear Risk of Bias, L = Low Risk of Bias.
Studies with unclear/high-risk ratings in ≥ 3 domains were considered weak, while those with < 3 were rated as fair.
3.3. Effect of AGE on Various Biomarkers of Cardiovascular Diseases
3.3.1. Systolic Blood Pressure (SBP)
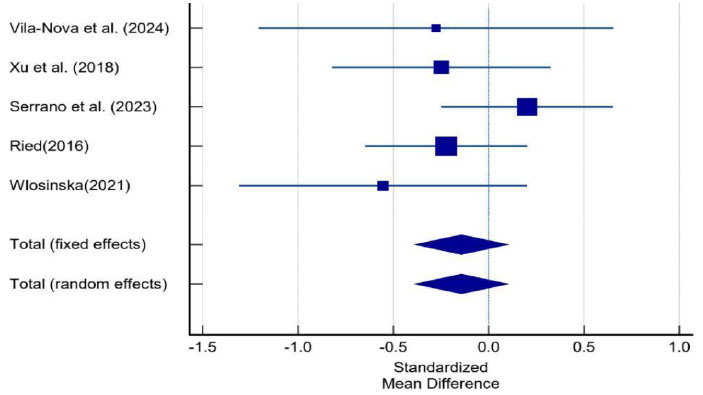
Nine studies with 11 effect sizes and 606 participants assessed the impact of AGE supplementation on SBP. Statistical analysis demonstrated a non-significant reduction of -1.71 mmHg in SBP levels following AGE administration (SMD: -0.15; 95% CI = −0.62, 0.32; p = 0.54). Substantial heterogeneity was observed (I2 = 87.39%, p < 0.001; Fig. 2). Subgroup analyses revealed differential effects based on dosage: trials using ≥ 1200 mg/day for 12 weeks showed a mean increase in SBP levels (+0.32 mmHg), while those with lower dosages (< 1200mg/day) demonstrated a significant decrease (-1.25 mmHg).
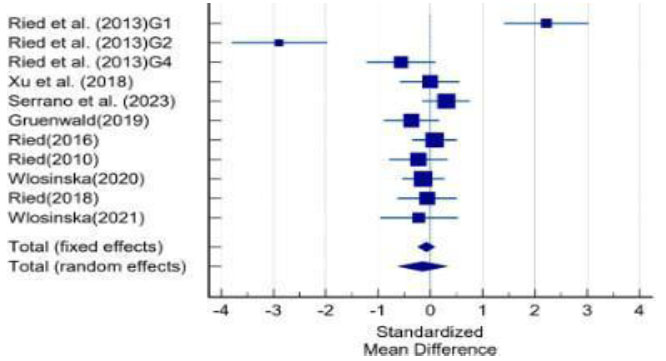
Forest plot showing the effect of aged garlic extract (AGE) supplementation on systolic blood pressure (SBP) compared with placebo in randomized controlled trials.
3.3.2. Diastolic Blood Pressure (DBP)
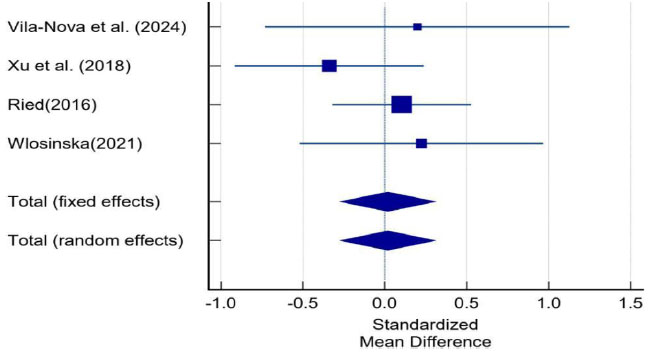
Nine studies with 11 effect sizes and 606 participants assessed the impact of AGE supplementation on DBP. Statistical analysis demonstrated a non-significant reduction of -0.77 mmHg in DBP levels following AGE administration (SMD: -0.10; 95% CI = −0.35, 0.15; p = 0.44). Substantial heterogeneity was observed (I2: 50.32%; p = 0.66; Fig. 3). Subgroup analyses of trials with a 12-week duration demonstrated a significant mean DBP reduction of -0.42 mmHg for lower-dosage regimens (< 1200 mg/day), while those with higher dosages (≥ 1200 mg/day) demonstrated a non-significant decrease (-0.7 mmHg).
Forest plot showing the pooled effect of aged garlic extract (AGE) supplementation on diastolic blood pressure (DBP) compared with placebo.
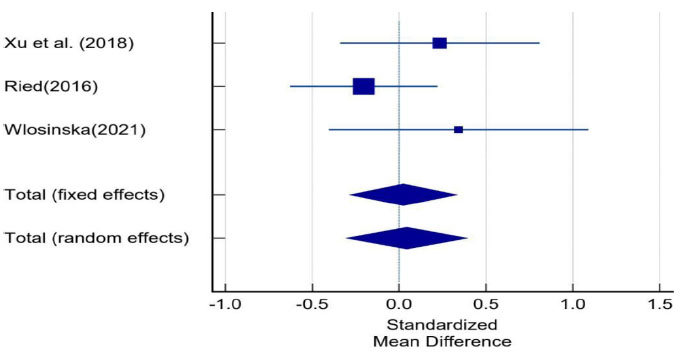
3.3.3. Pulse Pressure (PP)
Three studies (comprising 3 effect sizes and 214 participants) evaluated the effects of AGE supple-mentation on PP. The meta-analysis revealed a non-significant increase of + 1.60 mmHg in PP levels following AGE administration (SMD: 0.14; 95% CI: -0.13 to 0.41; p = 0.31). No significant heterogeneity was observed (I2 = 0.00%, p = 0.49; Fig. 4). Subgroup analyses of 12-week trials revealed a non-significant increase of +1.6 mmHg in PP levels with AGE dosages ≥ 1200 mg/day. Comparative data for lower dosages (< 1200 mg/day) at this duration were unavailable.
Forest plot illustrating the effect of aged garlic extract (AGE) supplementation on pulse pressure (PP) compared with placebo.
3.3.4. High-Density Lipoprotein Cholesterol (HDL-C)
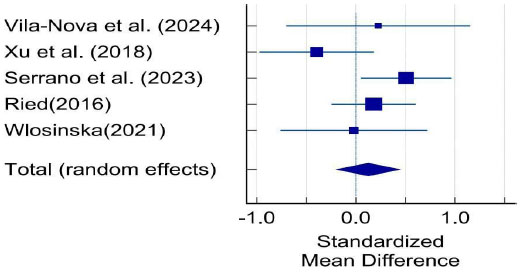
Five studies (5 effect sizes, N = 261 participants) evaluated the effect of AGE supplementation on HDL-C levels. The meta-analysis showed a non-significant increase of + 2.19 mg/dL in HDL-C levels following AGE administration (SMD: 0.16; 95% CI: -0.27 to 0.6; p = 0.45). Moderate heterogeneity was observed across studies (I2 = 64.65%, p = 0.02; Fig. 5).
Forest plot showing the effect of aged garlic extract (AGE) supplementation on high-density lipoprotein cholesterol (HDL-C) compared with placebo.
Subgroup analyses of 12-week trials revealed that AGE supplementation at ≥ 1200 mg/day produced a non-significant increase of + 5.52 mg/dL in HDL-C levels. Comparative data for lower dosages (< 1200 mg/day) were not available for analysis at this duration.
3.3.5. Low-Density Lipoprotein Cholesterol (LDL-C)
Four studies (4 effect sizes, N = 184 participants) evaluated the effect of AGE supplementation on LDL-C levels. The meta-analysis revealed a non-significant increase of + 0.65 mg/dL in LDL- C levels following AGE administration (SMD: 0.02; 95% CI: -0.27 to 0.31; p = 0.9), with no observed heterogeneity (I2 = 0.00%, p = 0.53; Fig. 6). Subgroup analyses of 12-week trials showed that AGE supplementation at ≥ 1200 mg/day produced a non-significant LDL-C reduction (-3.55 mg/dL). Comparative data for lower dosages (< 1200 mg/day) were not available for analysis at this duration.
Forest plot depicting the effect of aged garlic extract (AGE) supplementation on low-density lipoprotein cholesterol (LDL-C) compared with placebo.
3.3.5.1. Triglycerides (TG)
Five studies (5 effect sizes, N = 261 participants) evaluated the effect of AGE supplementation on TG levels. The meta-analysis showed a non-significant decrease of -22.08 mg/dL in TG levels following AGE administration (SMD: -0.14; 95% CI: -0.39 to 0.01; p = 0.24). No significant heterogeneity was observed across studies (I2 = 0.00%, p = 0.41; Fig. 7). Subgroup analyses demonstrated that trials with a duration of 12 weeks and a daily dosage of 1200 mg yielded a non-significant reduction of -4.61mg/dL in TG levels. Comparative data for lower dosages (< 1200 mg/day) were not available for analysis at this duration.
Forest plot illustrating the effect of aged garlic extract (AGE) supplementation on triglyceride (TG) levels compared with placebo.
3.3.5.2. Total Cholesterol (TC)
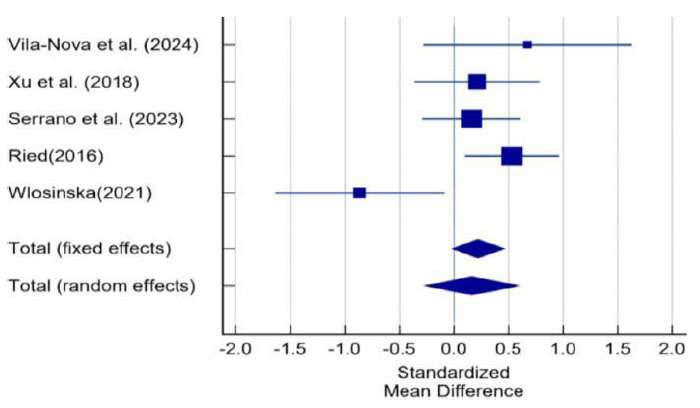
Five studies (comprising 5 effect sizes and 261 participants) examined the effect of AGE supplementation on TC levels. The meta-analysis showed a non -significant increase of 5.49 mg/dL in TC levels (SMD: 0.12; 95% CI: -0.19 to 0.44; p = 0.44), with moderate heterogeneity across studies (I2 = 36.82%; p = 0.18; Fig. 8). Subgroup analyses demonstrated that trials with a duration of 12 weeks and a daily dosage of ≥ 1200 mg yielded a non- significant increase of +16.43mg/dL in TC levels. Comparative data for lower dosages (< 1200 mg/day) were not available for analysis at this duration.
Forest plot showing the effect of aged garlic extract (AGE) supplementation on total cholesterol (TC) levels compared with placebo.
3.3.5.3. Non-High-Density Lipoprotein (Non-HDL-C)
Two studies (2 effect sizes, N = 67 participants) evaluated the effect of AGE supplementation on non-HDL-C levels. While the meta-analysis showed a non-significant reduction of -15.73 mg/dL in non-HDL-C levels (SMD: -1.49; 95% CI: -3.77 to 0.8; p = 0.12), considerable heterogeneity was observed across studies (I2 = 93.36%, p = 0.001; Fig. 9). No data were available for subgroup analysis.
Forest plot depicting the effect of aged garlic extract (AGE) supplementation on non-high-density lipoprotein cholesterol (non-HDL-C) compared with placebo.
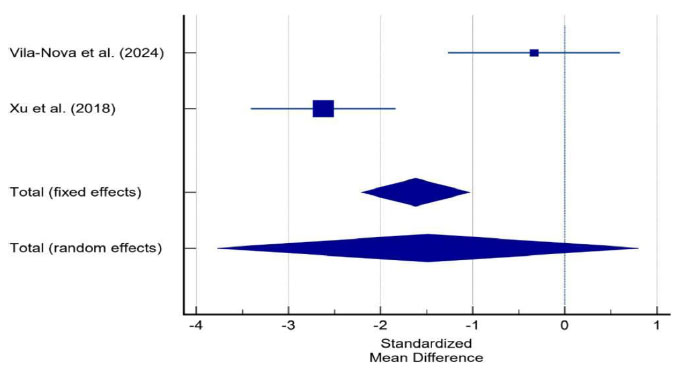
3.3.5.4. Tumor Necrosis Factor-alpha (TNF-α)
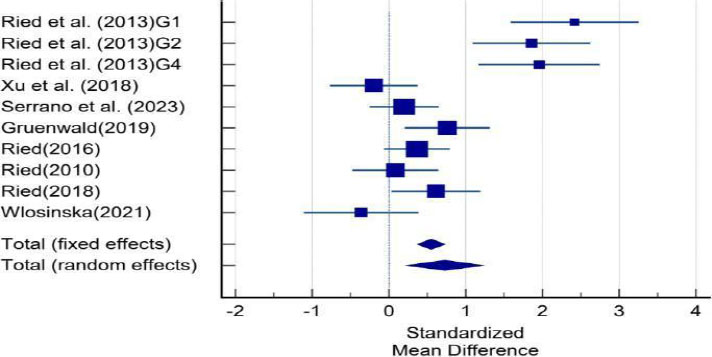
Three studies (3 effect sizes, N = 185 participants) evaluated the effect of AGE supplementation on TNF-α levels. The meta-analysis demonstrated a significant reduction of -178.62 fg/mL in TNF- α concentrations following AGE administration (SMD: -0.486; 95% CI: -0.90 to -0.07; p =0.02). Moderate heterogeneity was observed across studies (I2 = 47.3%, p = 0.15; Fig. 10). Subgroup analyses demonstrated that trials with a duration of 12 weeks and a daily dosage of ≥ 1200 mg yielded a non-significant reduction of -120.1 fg/ml in TNF-α levels. Comparative data for lower dosages (< 1200 mg/day) were not available for analysis at this duration.
Forest plot illustrating the effect of aged garlic extract (AGE) supplementation on tumor necrosis factor-alpha (TNF-α) concentrations compared with placebo.
3.3.5.5. Interleukin-6 (IL-6)
Three studies (3 effect sizes, N = 126 participants) evaluated the effect of Aged Garlic Extract (AGE) supplementation on Interleukin-6 (IL-6) levels. In contrast, the meta-analysis demonstrated a non-significant reduction of -469.5 fg/mL in IL-6 concentrations (SMD: -0.54; 95% CI: -2.14 to 1.05; p = 0.5). Substantial heterogeneity was observed across studies (I2 = 93.03%, p = 0.002; Fig. 11). No data were available for subgroup analysis.
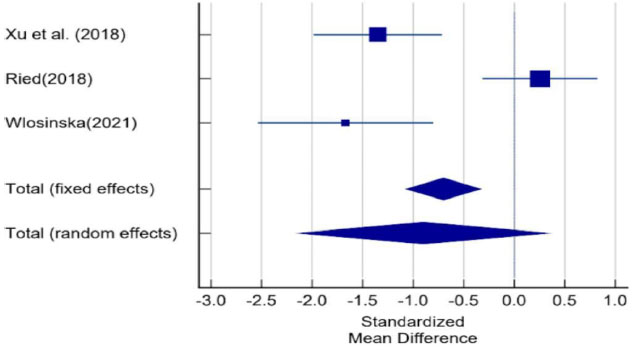
Forest plot showing the effect of aged garlic extract (AGE) supplementation on interleukin-6 (IL-6) concentrations compared with placebo.
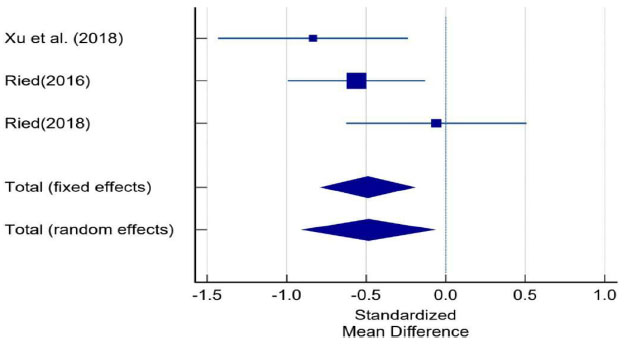
3.3.5.6. C-reactive Protein (CRP)
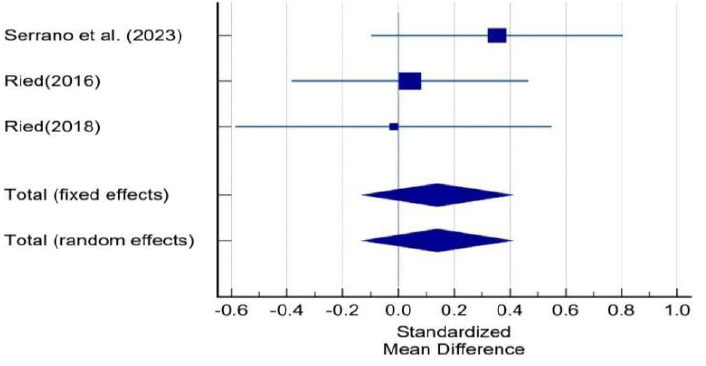
Three studies (3 effect sizes, N = 126 participants) evaluated the effect of AGE supplementation on CRP levels. The meta-analysis showed a non-significant change of +0.029 mg/dL in CRP concentrations following AGE administration (SMD: 0.04; 95% CI: -0.3 to 0.390; p = 0.8). Low heterogeneity was observed across studies (I2 = 18.08%, p = 0.29; Fig. 12). No data were available for subgrsoup analysis.
Forest plot depicting the effect of aged garlic extract (AGE) supplementation on C-reactive protein (CRP) concentrations compared with placebo.
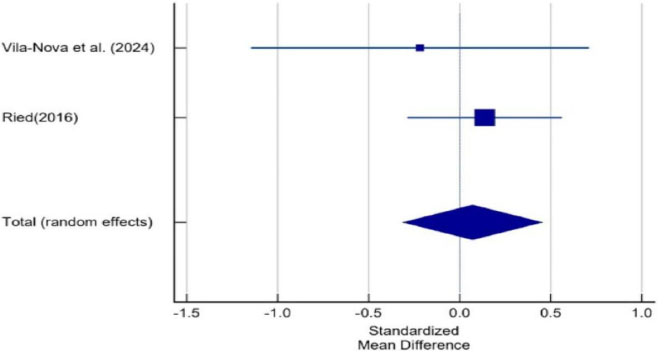
3.3.5.7. Blood Glucose (BG)
Two studies (2 effect sizes, N = 107) evaluated the effects of Aged Garlic Extract (AGE) on BG levels. The meta-analysis showed a non-significant increase of + 1.57 mg/dL in BG levels (SMD: 0.11; 95% CI: -0.18 to 0.4; p = 0.46), with no heterogeneity observed (I2 = 0.00%, p = 0.86). In subgroup analyses, higher-dose regimens (≥ 1200 mg/day for 12 weeks) were associated with a modest BG increase (+ 1.29 mg/dL) (Fig. 13). Comparative data for lower dosages (< 1200 mg/day) were not available for analysis at this duration.
Forest plot illustrating the effect of aged garlic extract (AGE) supplementation on blood glucose (BG) levels compared with placebo.
3.3.5.8. Arterial Stiffness (Augmentation Index: AI@75%)
Three studies (3 effect sizes, N = 220) evaluated the effects of AGE on AI levels. The meta-analysis showed a non-significant increase of +4.71% in AI levels (SMD: 0.06; 95% CI =−0.35, 0.47; p = 0.77; I2: 57.67%; p = 0.09), with no heterogeneity observed (I2 = 0.00%, p = 0.86). In subgroup analyses, higher-dose regimens (≥ 1200 mg/day for 12 weeks) were associated with a non-significant AI increase (+ 0.85%) (Fig. 14). Comparative data for lower dosages (< 1200 mg/day) were not available for analysis at this duration.
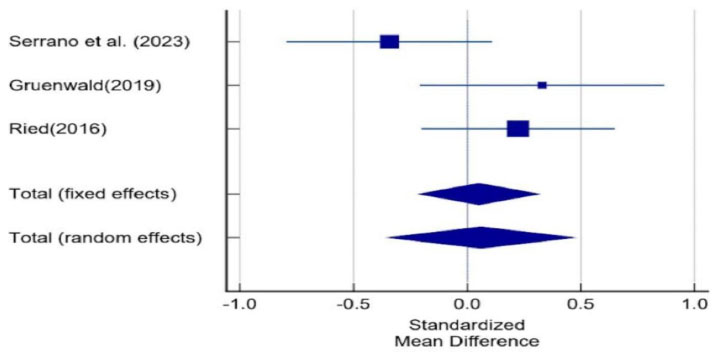
Forest plot illustrating the pooled effect of aged garlic extract (AGE) supplementation on arterial stiffness, measured as the augmentation index corrected to a heart rate of 75 beats/min (AI@75), compared with placebo.
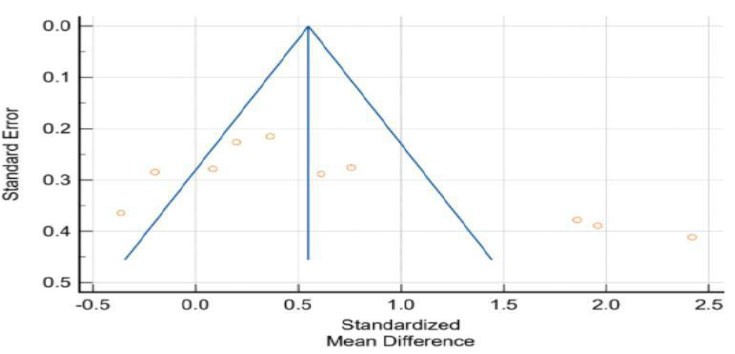
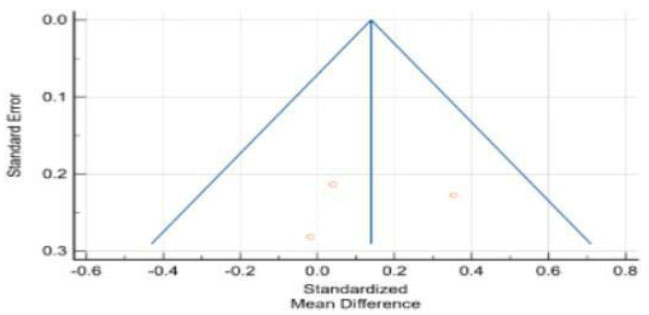
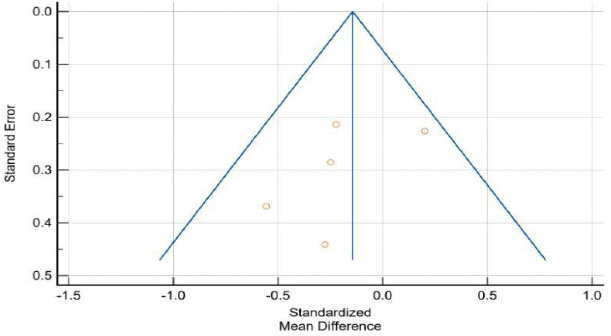
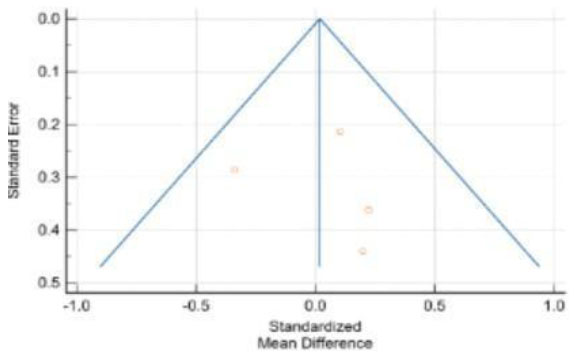
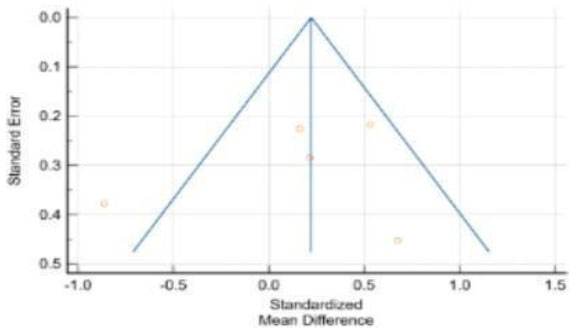
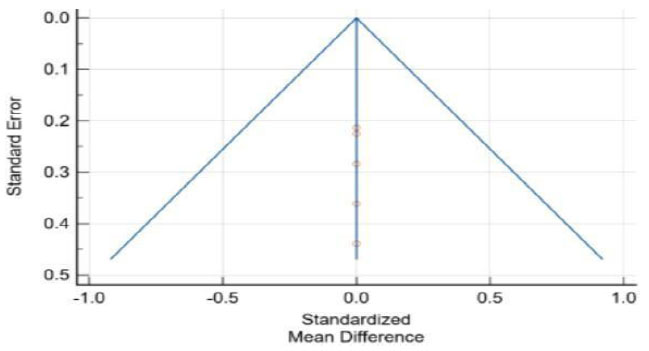
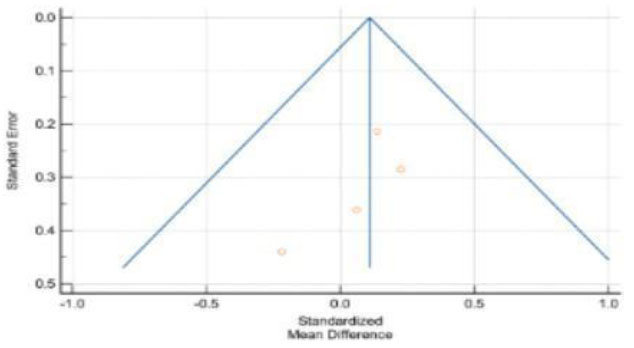
3.3.6. Publication Bias
Analysis of the funnel plots (Figs. 15-27) demonstrated relative symmetry, indicating a low probability of significant publication bias for the primary outcomes. However, the robustness of the combined effect varied considerably across heterogeneity levels. Substantial heterogeneity was observed for key cardiovascular metrics, including SBP, Non-HDL-C, and IL-6, suggesting that the pooled non-significant estimates for these factors are sensitive to inter-trial variation. Conversely, the neutral effect sizes for LDL-C, CRP, PP, BG, and TG were highly consistent across all studies.
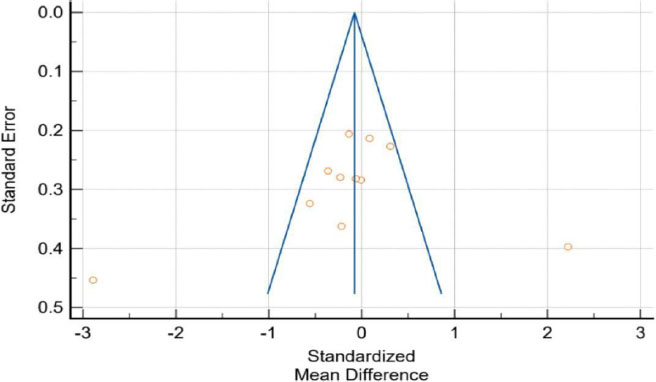
Funnel plot evaluating potential publication bias for studies included in the meta-analysis of systolic blood pressure (SBP). Symmetry of the distribution indicates a low likelihood of publication bias.
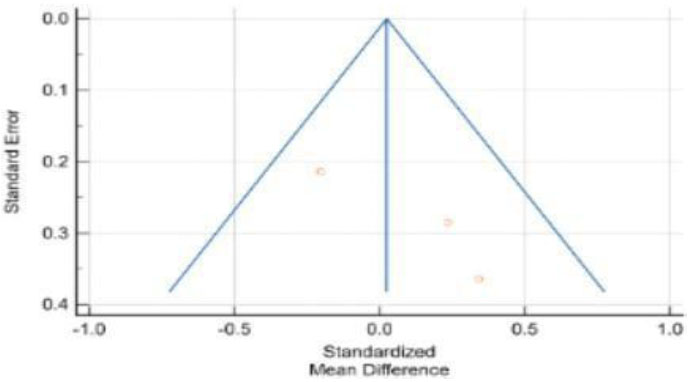
Funnel plot assessing publication bias for studies evaluating diastolic blood pressure (DBP) following aged garlic extract supplementation.
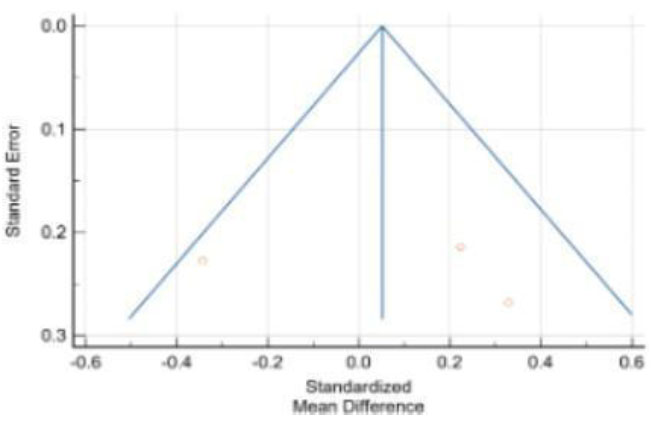
Funnel plot evaluating publication bias for studies included in the meta-analysis of pulse pressure (PP).
Funnel plot assessing publication bias for studies evaluating high-density lipoprotein cholesterol (HDL-C).
Funnel plot evaluating publication bias for studies included in the meta-analysis of low-density lipoprotein cholesterol (LDL-C).
Funnel plot assessing publication bias for studies evaluating triglyceride (TG) concentrations.
Funnel plot evaluating publication bias for studies included in the meta-analysis of total cholesterol (TC).
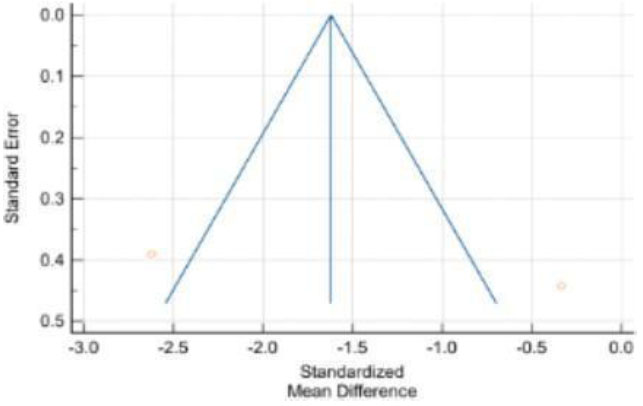
Funnel plot assessing publication bias for studies evaluating non-high-density lipoprotein cholesterol (Non-HDL-C).
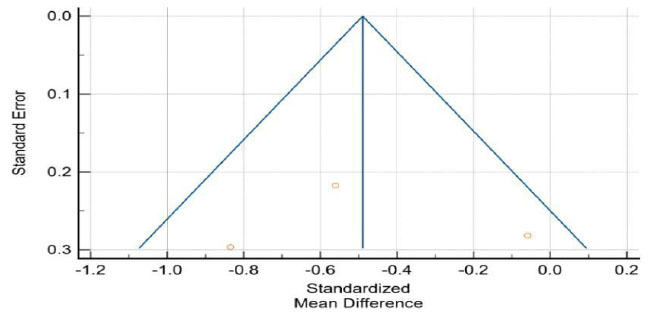
Funnel plot evaluating publication bias for studies included in the meta-analysis of tumor necrosis factor-alpha (TNF-α).
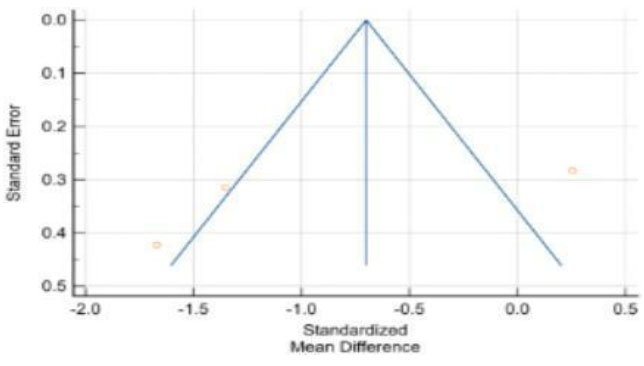
Funnel plot assessing publication bias for studies evaluating interleukin-6 (IL-6).
Funnel plot evaluating publication bias for studies included in the meta-analysis of C-reactive protein (CRP).
Funnel plot assessing publication bias for studies evaluating blood glucose (BG).
Funnel plot evaluating publication bias for studies included in the meta-analysis of arterial stiffness, measured as the augmentation index corrected to a heart rate of 75 beats/min (AI@75).
4. DISCUSSION
The trends we observed can be explained by the multiple biological effects of AGE, which contributes to cardiovascular health through interconnected effects. AGE's blood pressure–lowering effects can be attributed (at least in part) to increased Nitric Oxide (NO) activity, because AGE improves Endothelial Nitric Oxide Synthase (eNOS) activity, resulting in vasodilation and reduced vascular resistance [23-25]. Sulfur-containing compounds, when metabolized (including S-allylcysteine (SAC)), produce hydrogen sulfide (H2S), a major regulator of vascular tone and blood flow [26, 27]. Moreover, AGE might also modestly inhibit Angiotensin-Converting Enzyme (ACE), further contributing to blood pressure regulation [28-30]. AGE also affects lipid metabolism by inhibiting 3-Hydroxy 3-Methyl Glutaryl Coenzyme A (HMG-CoA) reductase (the enzyme responsible for hepatic cholesterol synthesis) to lower LDL-C and total cholesterol [31-33]. AGE may also facilitate improved reverse cholesterol transport due to upregulation of ABCA1 transporters that produce increased HDL-C concentrations [34, 35]. The antioxidant constituents of AGE (e.g., DACS) may also protect LDL-C from oxidative damage and should improve the quality of the lipid profile, oxidative stress, and progression of atherosclerosis [36-38]. In terms of inflammation, AGE has been shown to down-regulate NF-kB signaling, resulting in decreased pro-inflammatory cytokines such as TNF-α and IL-6 [24]. It can also upregulate the induction of Heme Oxygenase-1 (HO-1), which seeks to reduce oxidative stress and inflammation [16, 39]; and its sulfur amino acids (e.g., SAC, SAMC) may also be involved in inhibiting the MAP kinase (MAPK) pathway and inflammatory gene expression [40]. These factors likely explain the reduction in TNF-α and the slight reductions in IL-6 and CRP levels that were observed [41]. While there were no statistically significant changes in glycemic measures, AGE may help with enhancing insulin sensitivity and glucose uptake by decreasing oxidative stress and exerting a protective effect on pancreatic cells [42]. These effects are more significant in those with insulin resistance and poor glycemic control, and/or in those using higher doses and longer durations [43, 44]. Finally, AGE also promotes vascular health through maintenance of endothelial function, decreased arterial stiffness, and decreased vascular calcification due to improved NO signaling and reduced oxidative stress [45]. Collectively, these mechanisms, such as vasodilation, lipid regulation, anti-inflammatory and antioxidant effects, and/or vascular protective effects, provide a strong biological basis for the cardioprotective effects in this meta-analysis [46].
5. LIMITATIONS AND FUTURE DIRECTIONS
While this review and meta-analysis offer valuable insights into the cardiovascular effects of Aged Garlic Extract (AGE), several limitations should be noted. First, there was significant variation among the studies included, especially regarding blood pressure and lipid outcomes. This variation likely stems from differences in study design, the length of the intervention, AGE formulations (such as capsule, powder, or liquid), and dosage levels (which ranged from less than 600 mg/day to more than 2400 mg/day). The lack of standardized dosing regimens makes it difficult to compare results directly and limits the ability to identify an optimal dose. Second, the sample sizes were generally small, with most trials having fewer than 100 participants. These smaller studies increase the risk of type II errors and may miss clinically significant effects. Additionally, some trials included mixed populations (normotensive, hypertensive, or subjects with metabolic syndrome), which introduces potential confounding variables that limit the applicability of results. Third, variability in how outcomes were reported, for instance, inconsistent units or lack of baseline adjustments, limited the depth of the quantitative analysis. Few studies have examined secondary endpoints like endothelial function, oxidative biomarkers, or vascular stiffness using standardized methods. This variability may also indicate publication bias, as smaller studies with null results are less likely to appear in research databases. Fourth, the short duration of interventions (typically 6 to 12 weeks) may not be sufficient to capture long-term cardiovascular effects, particularly for outcomes like arterial stiffness, atherosclerosis progression, or lipid turnover. We need studies that continue for over 12 months to assess ongoing effectiveness and safety. Fifth, several included trials did not adequately report blinding or the allocation method, which poses risks of performance and detection bias. Moreover, most trials did not provide detailed assessments of participant compliance or validate biomarkers of AGE intake, creating uncertainty about actual exposure levels. Finally, our review did not study pharmacogenomic or microbiome-related interactions that could affect AGE bioavailability and variability in response. Emerging evidence indicates that the composition of the gut microbiota may influence the production of garlic metabolites, underscoring the need for further study of these mechanisms.
Overall, while this meta-analysis supports the biological plausibility and modest clinical benefits of AGE, these limitations highlight the need for well-designed, larger, multicenter randomized controlled trials. Future research should use standardized dosing protocols, include a variety of populations, focus on long-term outcomes, and integrate mechanistic biomarkers to clarify AGE's exact role in preventing and treating cardiovascular issues.
CONCLUSION
This systematic review and meta-analysis of 10 randomized controlled trials involving 625 participants found that supplementation with Aged Garlic Extract (AGE) may provide measurable cardiovascular benefits, although the effect is dose-dependent. The meta-analyses found significant reductions in systolic blood pressure (-1.71 mmHg) and diastolic blood pressure (-0.77 mmHg), significant reductions in triglycerides (-22.08 mg/dL) and Non-HDL-C (-15.73 mg/dL), a non-significant reduction in IL-6 (-469.5 fg/mL), and a significant reduction in TNF-α (-178.62 fg/mL). The effects on the lipids, which were more modest, appear to be beneficial especially with higher doses (≥ 1200mg) of +5.52 mg/dL non-significant increase in HDL cholesterol and a -3.55 mg/dL non-significant decrease in LDL cholesterol at higher doses. However, high variability between studies (especially for BP outcomes) suggests that individuals may respond differently based on baseline characteristics or formulations. Finally, AGE had no significant effects on total cholesterol, arterial stiffness, glucose metabolism, or C-Reactive Protein. Overall, these findings suggest that AGE could be a potential long-term complementary intervention for cardiovascular health with more focus on dosing approaches. Because of its robust adjunctive value, AGE (Aged Garlic Extract) can also be added to payloads of other supplements supported by evidence to provide potential additive benefits leading to better outcomes in ways that could (potentially) even be synergistic. As an adjunct therapy, AGE can enhance the benefits of cardiovascular, metabolic, and immune-enhancing supplements, making it a useful addition to integrative therapy approaches. Clinical trials indicate that AGE has been shown to reduce the progression of atherosclerosis when taken with B vitamins and L-arginine, improve outcomes for oxidative biomarkers and vascular function [47], while attenuating the accumulation of fat in adipose tissues of patients at risk for metabolic disorders [46]. The supplement has also been shown to improve adiponectin levels in patients with metabolic syndrome [47, 48], improve immune functioning, including phagocytosis [49], and enhance cardiovascular and gut health outcomes in individuals diagnosed with hypertension [50]. Current evidence supports the role of AGE in combination therapies, while warranting future research to validate a dosing standard and evaluate clinical long-term outcomes associated with clinical implementation. Dosing standards are especially critical to the high-risk population (hypertensive, hyperlipidemic, immunocompromised) that can potentially benefit the most from adjunctive supplementation strategies. Future studies should also consider the potential significance of AGE combined with other bioactive compounds to maximize its adjunctive potential in practice [51-53].
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: S.M.: Conceptualized and designed the study, supervised the project, allocated work, and critically revised the manuscript; A.A.R., A.U.A., R.D., and S.D.: Conducted the literature search, performed study selection and screening according to PRISMA guidelines, collected data, and carried out the data analysis; H.A.: Provided expert guidance in meta-analysis and co-supervised the study; A.H.M.R.: Assisted with statistical analysis, reviewed the manuscript, and verified the data. All authors read and approved the final manuscript.
LIST OF ABBREVIATIONS
| ACE | = Angiotensin Converting Enzyme |
| AGE | = Aged Garlic Extract |
| AI@75 | = Augmentation Index at 75% |
| BMI | = Body Mass Index |
| BG | = Blood Glucose |
| CI | = Confidence Interval |
| CRP | = C-Reactive Protein |
| CVD | = Cardiovascular Diseases |
| DBP | = Diastolic Blood Pressure |
| eNOS | = Endothelial Nitric Oxide Synthase |
| HDLC | = High-Density Lipoprotein-Cholesterol |
| HMG CoA | = 3-Hydroxy 3-Methyl Glutaryl Coenzyme A |
| HO-1 | = Heme Oxygenase- 1 |
| IL-6 | = Interlukin-6 |
| I2 | = Heterogenity Index(I-Squared Statistics) |
| LDL-C | = Low- Density Lipoprotein-Cholesterol |
| MAPK | = Mitogen-Activated Protein Kinase |
| MeSH | = Medical Subject Headings |
| NF | = κB Nuclear Factor Kappa-Light-chain-enhancer of activated B cells |
| NO | = Nitric Oxide |
| Non-HDL-C | = Non–High-Density Lipoprotein Cholesterol |
| p-value | = Probability Value |
| PP | = Pulse Pressure |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analysis |
| RCT | = Randomized Controlled Trial |
| SAC | = S-Allyl Cysteine |
| SAMC | = S-Allyl Mercaptocysteine |
| SBP | = Systolic Blood Pressure |
| SD | = Standard Deviation |
| SMD | = Standardized Mean Difference |
| TC | = Total Cholesterol |
| TG | = Triglycerides |
| TNF-α | = Tumor Necrosis Factor-alpha |
| TLR | = Toll-like Receptor |
AVAILABILITY OF DATA AND MATERIALS
All the data and supporting material are available within the article.
ACKNOWLEDGEMENTS
The authors are grateful to the Biotechnology Department, RV College of Engineering, Bengaluru, India for providing valuable support during the research process.

